Experienced Legal Representation to Help You Seek Justice
Summary:
Bedsores are skin injuries resulting from continuous pressure on a body part. This skin breakdown can result in severe pain, infections, and early mortality. Our nursing home bedsore attorneys can analyze the injury timeline and identify potential neglect to help you secure compensation. Contact us for a free consultation.
What Are Bedsores?
Bedsores, also called pressure sores or decubitus ulcers, occur when hospitals and nursing homes leave a patient in the same position for prolonged periods, cutting off blood flow and damaging the skin and underlying tissue.
Although largely preventable with adequate care, bedsores are a persistent issue in nursing homes and often signal neglect or abuse. If the assisted living facility or nursing home your loved one is in has failed to prevent this serious health complication, you must seek legal assistance from skilled personal injury attorneys.
What Are Common Causes of Pressure Ulcers in Nursing Homes?
Inadequate Staffing: Many nursing homes suffer from understaffing or a lack of adequately trained staff, making it challenging to provide each resident with the necessary care. When nursing homes are inadequately staffed, patients may not receive the repositioning, hygiene, or monitoring needed for bedsore prevention.
Failure to Reposition Patients: One of the most important preventive measures for avoiding sores is regularly changing the position of immobile residents. Nursing homes that fail to implement these practices increase the risk of pressure ulcer development, often due to staff neglect and medical malpractice.
Missed Repositioning or Offloading: Inattentive staff may reposition a patient but fail to place them in an offloading position, thereby not relieving pressure on the vulnerable area.
Negligent Moisture Management: Ulcers must be kept clean and dry to allow the skin barrier to heal. Leaving bandages on for too long, not drying the area after bathing, or leaving residents in wet clothing can all lead to infections and worsened skin breakdown.
Delayed Escalation or Wound Consult: If a resident shows early signs of a pressure ulcer, such as red spots that do not blanch when pressed, nursing staff should notify a physician and request a wound care consultation. Failure to do so can be negligence.
What Are the Risk Factors for Developing Pressure Ulcers?
Vulnerable patients should receive assessments and careful monitoring. Individuals with certain medical conditions or who receive inadequate care are at a higher risk of skin issues.
Limited Mobility: A mobile resident can reposition themselves to avoid prolonged pressure on a certain body part, whether that is their coccyx or heels. However, immobile patients depend entirely on nursing staff to help them reposition as necessary, making them vulnerable to pressure ulcers from neglect.
Vascular Disease: Ulcers occur when there is decreased blood flow to an affected area, causing tissue death. Individuals with vascular issues may develop sores faster, and these sores may not heal as easily.
Poor Hygiene: If nursing home staff members do not ensure the resident remains clean and dry, there is a significant risk of bedsores developing.
Diabetes: Chronically high blood sugar can damage the immune system and reduce nerve signaling, especially in the feet. Diabetic foot ulcers may go unnoticed for a significant period of time because the resident no longer feels sensation in the area.
Poor Nutrition: Malnourished nursing home residents may develop ulcers because their skin barrier is not getting the nutrients it needs to rebuild, and their immune system cannot fight off small infections.
If left untreated, a bed sore can lead to a range of severe and life-threatening complications. The progression of a pressure ulcer can result in these concerns.
Cellulitis: Open wounds from bedsores can become infected. If the infection spreads, it can lead to more severe conditions, such as a skin infection known as cellulitis.
Bacteremia: Infected pressure ulcers may introduce bacteria into the bloodstream. This can progress into sepsis, a systemic response to an infection.
Sepsis: One of the most dangerous complications of an untreated bed sore is sepsis, a life-threatening response to infection. Sepsis can cause organ failure and lead to death, making early intervention critical.
Cancer: When pressure ulcers do not heal, they may becomeMarjolin’s ulcers, which can be a precursor to squamous cell carcinoma.
Septic Arthritis: Infected sores can also spread bacteria to joints. Septic arthritis is debilitating and can lead to permanent damage, including reduced mobility.
How a Nursing Home Bed Sore Lawyer Can Help During the Legal Process
When a loved one developed pressure injuries due to nursing home neglect, pursuing legal action can feel overwhelming. A skilled nursing home bed sore attorney from our legal team can provide the legal expertise and support needed to navigate the legal system.
From investigating the case to taking it to trial, our dedicated pressure ulcer attorneys will work to hold the nursing home accountable and secure fair compensation for the harm caused.
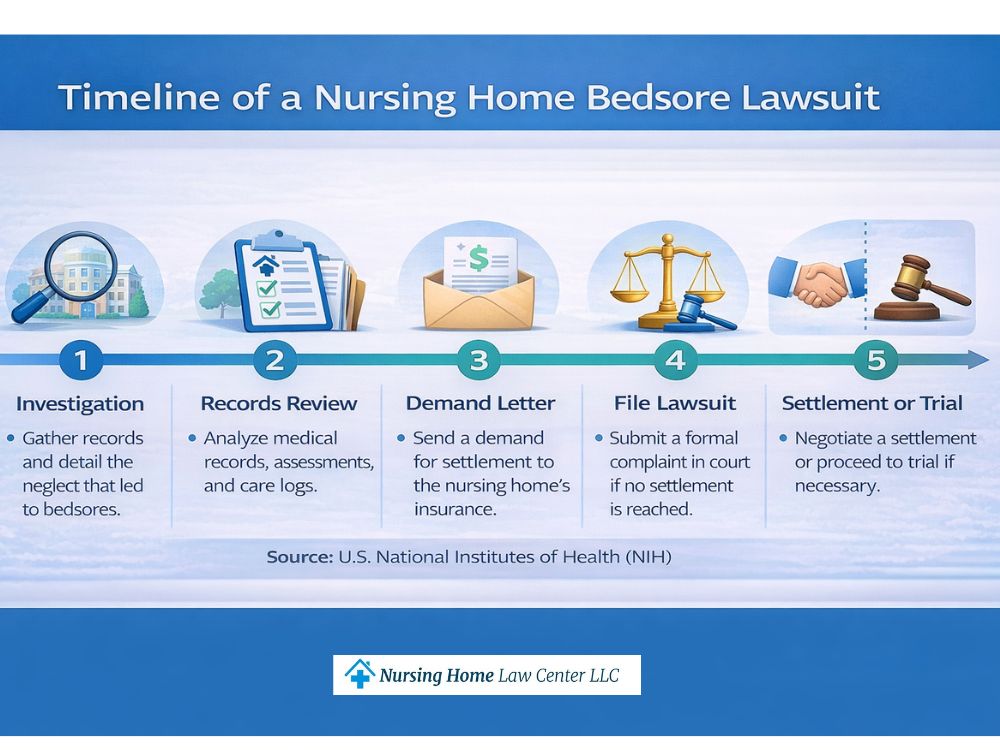
Investigating the Case
A pressure ulcer lawyer from our team will thoroughly investigate the circumstances surrounding your loved one’s injury. This includes reviewing medical records, analyzing the nursing home’s care history, and identifying any instances of neglect or improper treatment.
By conducting a detailed investigation, our nursing home bedsore attorneys can build a strong case demonstrating the facility’s failure to provide adequate care.
Gathering and Preserving Evidence
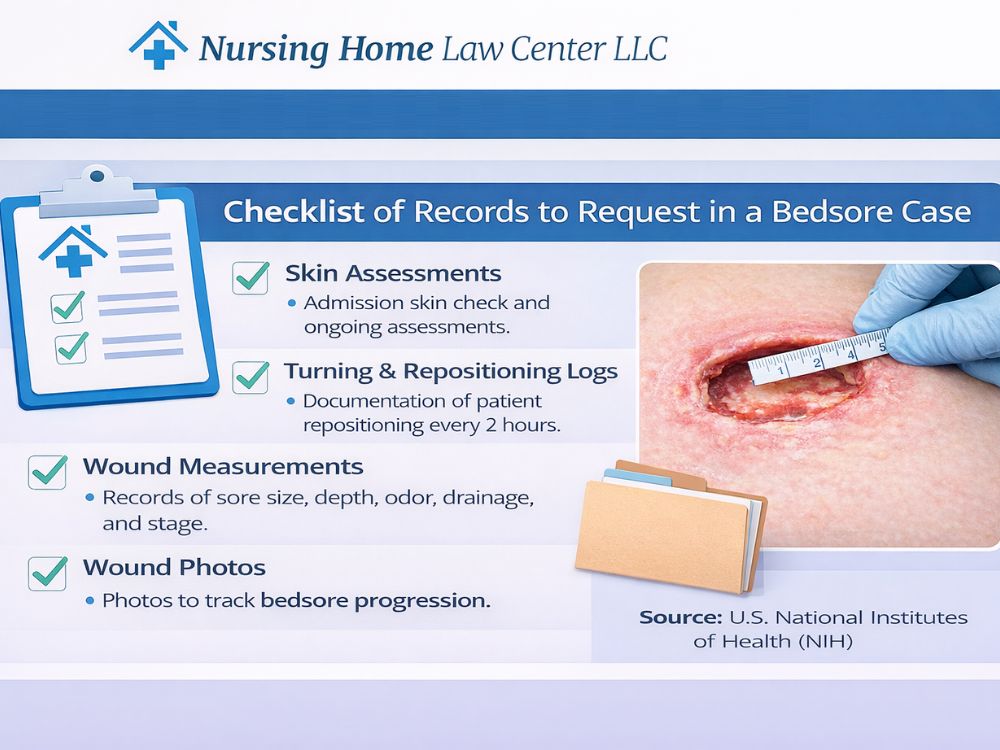
Our personal injury lawyers will request that any evidence connected to your loved one’s case be preserved by the facility and any hospitals they visited. Evidence that can support your claim includes:
Skin integrity assessments
Skin checks
Turning logs
Wound photos
Wound measurements
Pharmacy orders for topicals, dressings, and antibiotics
Medical Administration Record (MARs) for medication applications
Wound care logs
Witness statements
This evidence can be used to develop a timeline of events and demonstrate whether the facility adhered to the expected standards of care in wound treatment.
Calculating Damages for a Fair Settlement
Before we negotiate with the facility’s insurance carrier, it’s important to know the full scope of your economic and non-economic damages.
Economic damages cover hard financial losses like medical bills, surgeries, rehabilitation, and estimates for future care needs. If your loved one passed away due to medical neglect, burial and funeral costs can be included.
Non-economic damages consider the emotional and physical impact, such as pain and suffering, and emotional distress. These are typically calculated in relation to the economic damages.
Negotiating with Insurance Companies
Nursing homes and insurance companies often attempt to minimize payouts in bedsore cases. An experienced nursing home bedsore lawyer from our team will negotiate with insurance companies on your behalf, ensuring you receive a fair settlement covering all medical expenses, pain and suffering, and other damages.
We will use their expertise to push back against lowball offers and seek the compensation you deserve.
Bedsore Litigation in Court
If a fair settlement cannot be reached through negotiations, we will be prepared to take the case to trial. Our skilled nursing home pressure sore lawyers will present the evidence, call upon expert witnesses, and argue your case before a judge or jury to seek maximum compensation for your loved one’s suffering.
How to File a Nursing Home Bed Sore Lawsuit
Acting quickly is essential to protecting your loved one and building a strong case. Follow these steps as soon as possible.
Remove your loved one from the negligent institution.
Get medical care for the pressure ulcer at a local hospital.
Take photos of the pressure injuries.
Preserve any available evidence, such as medications or creams that were used.
Request the resident’s records from the nursing home facility.
Contact an attorney for a free case review and learn more about your legal options.
What Compensation Is Awarded in Nursing Home Abuse Cases Involving Bedsores?
When a resident suffers from bedsores due to neglect or improper care, the law allows victims and their families to seek financial compensation for the harm caused. The compensation awarded typically falls into several categories, each designed to address different aspects of the suffering and losses incurred.
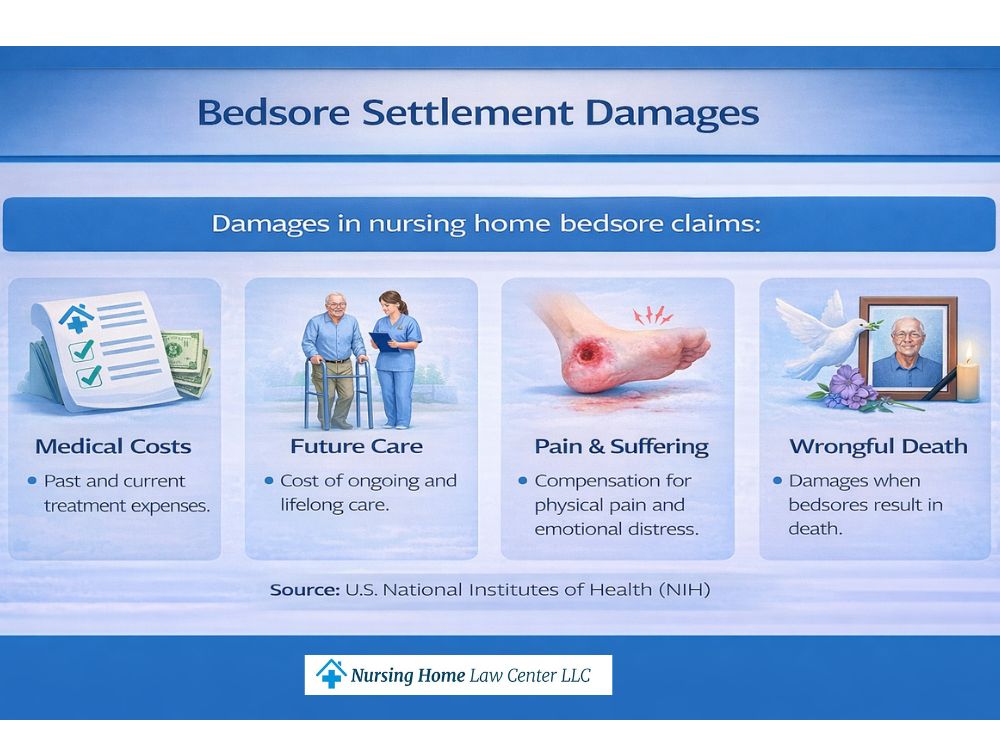
Economic Damages
Economic damages cover the direct financial costs associated with developing and treating bedsores. These damages often include medical expenses, long-term care, and other costs tied to the resident’s recovery.
Non-Economic Damages
Non-economic damages address the emotional and physical suffering caused by the development of bedsores. This can include compensation for pain and suffering, loss of quality of life, and the psychological toll the injuries have taken on the resident.
Punitive Damages
In cases where the nursing home’s neglect was particularly egregious or intentional, punitive damages may be awarded. These damages are meant to punish the facility for its conduct and deter similar behavior in the future.
Wrongful Death Damages
If a resident dies due to complications from untreated bedsores, the family may be entitled to damages for funeral expenses, loss of companionship, and other related costs.
What Is the Average Payout for Nursing Home Decubitus Ulcers?
Payouts in nursing home bedsore cases range from $55,169 to $114,000,000. The average payout is $6,116,979, while the median recovery is $1,000,000.
Several factors can influence the value of a claim, including:
Stage and severity of the bedsore and whether a serious infection, amputation, or death occurred
Resident’s age, overall health, and life expectancy
Whether the injury was preventable through repositioning, monitoring, or staff intervention
Documentation of care plans, wound treatment, and whether records were falsified or incomplete
Timing and quality of medical care provided once the sore was identified
Evidence of systemic understaffing, poor training, or neglectful supervision
Testimony from medical and nursing experts on causation and standard of care
Settlements Recovered by Our Experienced Attorneys
$12,800,000: Marcy was a long-term nursing home resident with a high body weight and significant mobility challenges who required regular repositioning. The facility left her prone for extended periods of time and also failed to prevent bedsores. Marcy passed away from bacteremia due to nursing home negligence.
$3,245,000: Roger was admitted to a long-term hospital after a traumatic brain injury. Instead of receiving quality treatment, he developed multiple decubitis ulcers on his heels, hips, and coccyx that resulted in severe infections.
$2,150,000: Alan was in a skilled nursing facility while recovering from a fractured hip. Nurses refused to help him with his hygiene, causing a bed sore that evolved into sepsis. His family sued for wrongful death, and the facility settled out of court.
Seek Legal Support from the Nursing Home Law Center
The team at Nursing Home Law Center has secured over $450 million for injured clients and their loved ones during the past 25 years. As proud members of the American Association for Justice and the Million Dollar Advocates Forum, our team has over 100 years of combined legal experience.
We understand the significant financial and emotional stress that nursing home negligence can cause. Our compassionate attorneys will guide you through every step of the legal process and communicate with third parties on your behalf. We take cases on a contingency fee basis, meaning you owe us nothing unless we earn compensation for you.
How Common Are Bedsores in Nursing Homes and Assisted Living Facilities?
Pressure sores are considered a “never event” in healthcare settings, meaning they should never develop under proper care and supervision. Unfortunately, they happen with disturbing frequency in nursing homes across the country.
According to the Centers for Disease Control and Prevention (CDC), over 10% of nursing home patients suffer from pressure sores. Approximately half of these cases are classified as Stage III or Stage IV, severe wounds involving deep tissue damage and increased risk of infection. Of those with serious wounds, 60% of patients will die within a year of developing pressure sores.
Patients with untreated pressure ulcers are 2 to 6 times more likely to die from complications compared to other severe health conditions, such as cardiovascular disease and cancer. Sadly, only 35% of individuals who develop sores receive the treatment necessary to heal.
A single pressure ulcer can cost up to $37,800 to treat, placing a significant burden on families of negligent nursing home residents.
However, you do not have to face this alone. Our nursing home bedsore lawyers can help you secure compensation for the costs associated with pressure ulcers.
How Bedsore Stages Affect Lawsuits?
Bedsores progress through four stages, each representing increasing severity. These stages are critical in determining the strength and potential value of a bed sore lawsuit, as advanced stages often indicate prolonged neglect or nursing home abuse.
A pressure injury lawyer can help families understand the legal implications of each stage and seek justice for the harm caused.
Stage 1
This is the mildest form of a pressure ulcer, in which the skin appears red or discolored but remains intact. If treated promptly, a sore at this stage can heal quickly with no long-term damage. However, even a Stage 1 pressure sore can indicate nursing home neglect.
Stage 2
The skin begins to break open in this stage, forming a shallow wound. This stage may cause pain and expose the deeper layers of skin. Stage 2 bedsores are more concerning and suggest that proper preventive measures, such as repositioning and monitoring, have not been followed.
Stage 3
The pressure sores have progressed deeper, affecting the fatty tissue beneath the skin. The ulcer resembles a crater and increases the risk of infection. Stage 3 bedsores are often indicative of severe neglect and significantly increase the risk of long-term harm to nursing home patients.
Stage 4
This is the most severe stage, where the sore extends to the muscle and bone. Infection is common, and complications such as sepsis or death may result. Stage 4 bedsores are a clear indicator of extreme neglect, and lawsuits involving this stage typically result in higher compensation due to the severe harm caused.
As the sore progresses, the legal case becomes stronger. Advanced-stage pressure sores often signal extended neglect and can result in life-threatening conditions, directly impacting the potential compensation a family may receive in a bedsore lawsuit.
Unstageable Pressure Injury
An unstageable pressure injury cannot be sorted into the four stages because it is obscured by exudate, a protein-filled fluid that covers the wound. The exudate, or slough, keeps the wound moist but may also get infected. Because of this covering, clinicians cannot determine the injury’s depth. Because exudate only occurs with more severe tissue damage, its presence signifies negligence.
Deep Tissue Pressure Injury (DTPI)
A Deep Tissue Pressure Injury (DTPI) may look like a bruise at first, but it does not blanch when touched and has a different texture than the surrounding tissue. The skin may feel firm, mushy, or boggy. Like pressure ulcers, it results from prolonged pressure on a body part and affects deeper structures, such as at the bone-muscle interface. These injuries develop rapidly and may not be open wounds.
Book a Free Consultation to Explore Your Legal Options
If your loved one developed bedsores due to a healthcare provider’s negligence, you don’t have to face this battle alone.
At the Nursing Home Law Center, we have extensive experience handling cases involving decubitus ulcers and fighting for the rights of victims. Our law firm understands the unnecessary pain bedsores can cause and is committed to holding negligent nursing homes accountable.
Our dedicated team of nursing home bedsore lawyers is ready to help you pursue justice and secure the compensation your family deserves. We offer a free consultation to discuss your case and provide the guidance you need to take the next steps.
Don’t wait, and contact us today to learn how we can help you protect your loved one’s rights and seek financial compensation for their suffering. Let our nursing home abuse lawyers fight for the justice your family deserves. Call us or fill out our contact form.
FAQs
How do bedsores present themselves?
Understanding what bedsores look like at each stage will help you identify the early warning signs. A pressure ulcer begins as a discolored patch of skin that does not blanch when pressed. On light skin, it may look red, while on darker skin tones, it will be blue or purple. The skin may be swollen, unusually firm or soft, and warm to the touch.
Pain is one of the earliest pressure ulcer symptoms, often described as a burning or throbbing sensation even before any skin changes. When nursing home staff do not take resident complaints seriously, they may miss this key concern.
Where do pressure injuries typically occur?
Body parts where bedsores typically occur include heels, hips, buttocks, elbows, shoulders, and inner knees. Some residents may also suffer pressure ulcers on the back of the head if they are completely immobilized and cannot turn their head.
How are pressure ulcers treated?
Frequent repositioning is essential for pressure injury treatment and prevention. Nursing staff should rotate residents frequently so that pressure is dispersed throughout the body rather than concentrated in one place.
If a pressure ulcer begins to develop, staff should develop a bedsore wound care plan for the resident that includes cleaning and dressing the injury. This can include DuoDERM, a hydrocolloid dressing that helps remove dead tissue and improve skin health without requiring surgical intervention.
Some residents will need pressure ulcer debridement, which removes dead tissue and encourages cell turnover. This can be done through topical enzymes or mechanical debridement, which are specialized pads that rub away the tissue. In severe cases, surgical debridement may use a scalpel or scissors to cut necrotic tissue.
Can bedsores be prevented?
Nursing homes are expected to implement various preventive measures to reduce the risk of developing pressure injuries among residents. Some of the critical steps that should be taken include:
Regular repositioning to prevent constant pressure on vulnerable areas
Proper nutrition and hydration, which improve the skin barrier
Appropriate hygiene and skin care to ensure the resident’s well-being
Pressure-relieving devices, like specialized mattresses or cushions, that properly distribute pressure
Proper training to identify and treat bedsore injuries.
Do nursing homes have a legal duty to prevent pressure injuries?
Under 42 CFR § 483.25(c), nursing homes must ensure residents do not develop pressure ulcers unless they are clinically unavoidable. Demonstrating that the bedsores were avoidable and directly caused by the facility’s negligence is key to proving liability.
Who can file a bedsore lawsuit against a nursing home?
The nursing home or hospital resident has the legal right to file a claim against the negligent facility. If the person is deceased or incapacitated, a power of attorney also has the right to make medical and legal decisions for the resident.
Some individuals do not name a power of attorney before they become incapacitated or pass away. In this case, the next of kin or a legal guardian, like an appointed attorney, can file on their behalf.
What evidence is needed to support a nursing home bedsore case?
For a bedsore lawsuit to be successful, gathering strong evidence is essential. Some of the most critical pieces of evidence include:
Photographs of the affected area at different stages
Turning and repositioning logs
Nurse’s charts mentioning skin changes or resident complaints
Skin checks and assessments
Medical Administration Records (MARs) showing what was prescribed and when it was administered
Hospital admissions, if relevant
Wound care orders, like debridement
Witness statements from nurses and other residents
Nursing home communications with family members
Care plans that address family complaints
Preserving this evidence early is critical, as conditions can change rapidly. Collecting documentation, photos, and witness accounts as soon as possible increases the chances of building a solid case.
What are common defenses used by nursing homes in bed sore cases?
Nursing homes often employ various defenses when faced with bedsore lawsuits. The first is that the resident had pre-existing conditions, like immobility or diabetes, that caused unavoidable bedsores. However, federal and state regulations require nursing homes to take preventive measures. In many cases, bedsores are preventable even for those with pre-existing conditions.
The facility may also argue that the family denied necessary medical interventions. This is why it is crucial to keep records of all communications with the facility, as the communication records can disprove that the family refused medical care.
What is the role of expert witnesses in nursing home pressure ulcer cases?
Expert witnesses, such as medical professionals, can link the nursing home’s negligence to resident injuries by explaining factors that contribute to pressure ulcer development, such as failure to reposition or provide adequate nutrition.
One key aspect of medical testimony is that the professional can explain what a reasonably competent nurse or doctor would do when treating a patient with similar clinical signs. For example, they can explain how they would approach an immobile resident who complains of burning hip pain and has a non-blanching red spot. This opinion can be compared with the actual narrative of events to demonstrate the nursing home’s substandard care.
What is the statute of limitations for bed sore lawsuits against nursing facilities?
The statute of limitations is the legal time frame within which a nursing home lawsuit must be filed. Itvaries by state but typically ranges from one to three years from when the injury was discovered or should have been found.
Nursing home abuse lawsuits must be pursued according to the laws set forth by the state where the facility is located. In this section, our attorneys have compiled the relevant laws, regulations and local organizations for each state so you can get an idea of how the law impacts your situation. Should you decide to move forward with a case, you will also find information about locating an experienced attorney who can assist your family.
Jonathan did a great job helping my family navigate through a lengthy lawsuit involving my grandmother's death in a nursing home. Through every step of the case, Jonathan kept my family informed of the progression of the case. Although our case eventually settled at a mediation, I really was...
- Lisa
After I read Jonathan’s Nursing Home Blog, I decided to hire him to look into my wife’s treatment at a local nursing home. Jonathan did a great job explaining the process and the laws that apply to nursing homes. I immediately felt at ease and was glad to have him on my side. Though the lawsuit...